High cholesterol levels: Why taking your medicine diligently is more effective than changing your diet
A local study revealed medicine is 85 per cent effective compared to exercise and diet (10 per cent to 20 per cent). A doctor also breaks down misconceptions about statins, the most commonly prescribed medicine.



No one likes the idea of popping pills every morning. Take cholesterol-lowering medicines or statins, for example. To get themselves off the hook, many patients with high cholesterol levels tend to believe that diet changes and other lifestyle modifications alone would work.
Interestingly, when it comes to lowering cholesterol levels, being diligent with your medicine is far more beneficial than giving up wagyu beef. A local study by SingHealth Polyclinics (SHP) has found “adherence to medication to be the most critical factor” compared to other considerations such as ethnicity, diet, exercise and smoking.
Just how much more effective? Professor Tan Huay Cheem, a senior consultant with the Department of Cardiology at National University Heart Centre, Singapore, who isn’t part of the study, provided the breakdown below:
- Diet: 10 per cent to 20 per cent
- Exercise: 5 per cent
- Exercise and diet: 10 per cent to 20 per cent
- Medicine (oral): 30 per cent to 50 per cent
- Medicine (oral and injectable): Up to 85 per cent
Dr Tan Ngiap Chuan, who led the study and is the director of research at SHP, said the findings could prompt doctors to prioritise starting or adjusting medications with their patients. "We usually focus on other lifestyle factors first. We may switch the order now."

HOW DO THESE MEDICINES WORK?
In Singapore, nearly two out of 10 adults aged 18 to 69 have high cholesterol, according to the SHP study.
If you’re one of them, you’re probably put on statins (including atorvastatin and rosuvastatin), the most commonly prescribed medicine, said Prof Tan.
Statins are also known as HMG-CoA reductase inhibitors and they “work in the liver to prevent cholesterol from forming and reduce the amount of cholesterol circulating in the blood”.
“They are most effective at lowering LDL (bad) cholesterol, but also help to lower triglycerides and raise HDL (good) cholesterol,” said Prof Tan.
In addition to statins, a new class of injectables have emerged in recent years. They provide an alternative for patients “who are unable to achieve their targeted cholesterol levels, who are statin intolerant, or unable to adhere to regular therapies”, said Prof Tan.

These include the PCSK9 inhibitors (such as evolocumab and alirocumab), which are injected once every two weeks.
There are also the small interfering RNA or siRNA, which requires subcutaneous injection only once every six months. These siRNA include inclisiran, which was recently approved by Singapore’s Health Sciences Authority and the US Food and Drug Administration, said Prof Tan. “The injectables can be used in combination with oral medicines.”
Unfortunately, the commonly prescribed statins have received bad press on social media, said Prof Tan, even though they have been “proven to be effective in preventing heart attacks, strokes and death – even among low-risk patients”. It has led patients to develop “unfounded fears” for statin-associated side effects, he said.
Here, Prof Tan tackles some of the common misconceptions patients have about statins:
MISCONCEPTION 1: Doctors prescribe statins as a catch-all

Statins are widely used as they satisfy two crucial functions in disease management: Preventing the onset of disease before it begins; and reducing the severity or impact of a disease if it already has by “halting its progress and preventing recurrences”, said Prof Tan.
“Certainly, patients who are at low risk for heart attack and stroke will benefit less from taking statins,” he said. But “among medical experts, there is little debate on whether statins work in high-risk patients”.
Having said that, statins aren’t prescribed indiscriminately. According to Prof Tan, patients are usually started on a course only if they satisfy any of these criteria:
- Atherosclerotic cardiovascular disease. This means the patient has pre-existing blockages in the heart, brain or any arteries in the body’s circulatory system.
- Diabetes mellitus. Especially those who have been living with diabetes for more than 10 years.
- High LDL cholesterol level. Higher than 190mg/dL (4.9mmol/L).
- As prevention. These are patients with no established cardiovascular disease but have multiple risk factors that increase their chances of developing it in the future.
MISCONCEPTION 2: Once you start on statins, you have to be on them for life

This is true, though. The cholesterol-lowering benefits conferred by statins will only continue for as long as you take the medicine, said Prof Tan. “The cardio-protective effect is lost when the statins are stopped.” You would have considered to have discontinued your medication if you stopped for more than a year.
Perhaps the more pertinent question is: What are the effects of being on statins in the long run? “Studies have shown that statins are safe and well tolerated. They have been used for more than 30 years to lower cholesterol. In fact, statins work best when you take them for a long time,” said Prof Tan.
Look at it as insurance for a longer life and to prevent heart attacks and strokes, he added.
MISCONCEPTION 3: Statins cause diabetes

Statins have been found to slightly elevate blood sugar levels in clinical trials, said Prof Tan. And this creates the impression that statins can lead to diabetes.
“However, people experiencing this side effect are already prediabetic or have higher than normal blood sugar. For those who are borderline diabetic, this mild increase in blood sugar can lead to a diabetes diagnosis about five weeks earlier than it would be otherwise,” he said.
But if you’re not already predisposed to diabetes, that is, your blood sugar levels are normal, statins do not induce diabetes, said Prof Tan.
“Additionally, the benefits of reducing cardiac events in someone who has prediabetes or is diabetic greatly outweigh the slight increase in their blood sugar which may occur,” he said.
MISCONCEPTION 4: Statins destroy muscle tissue

The muscle-destroying conditions that you might have read about are known as myopathy and rhabdomyolysis. “Serious muscle damage such as myopathy and rhabdomyolysis are rare,” said Prof Tan.
Myopathy refers to any disease that causes the muscles to lose control, leading to muscle weakness. Rhabdomyolysis, on the other hand, results from the disintegration of the muscle fibres. Both conditions have been linked to the frequent use of statins.
Prof Tan said that statin-associated muscle symptoms have been reported in studies in varying frequencies, from 10 per cent to 15 per cent in patients. However, he claimed that the incidence rate may be overestimated due to the nocebo effect.
The cardio-protective effect is lost when the statins are stopped. In fact, statins work best when you take them for a long time.
“This is when a patient with negative expectations of a medicine would experience its potential side effects at a much higher rate than he otherwise would,” said Prof Tan.
If you suspect you have statin-associated muscle symptoms, the ache and tenderness typically involve large muscle groups such as the shoulders and the thighs, and are usually bilateral. They also tend to be more pronounced after physical exercise, said Prof Tan.
Speak to your doctor who can put you on a different statin or reduce the dose, he said.
MISCONCEPTION 5: Statins do not really prevent vascular disease
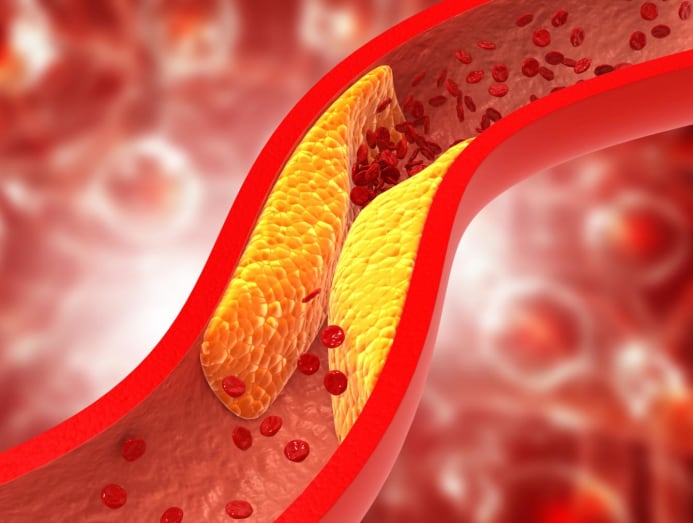
Vascular disease refers to any condition that affects the blood vessels in your body. As you’d already know, having a high cholesterol level means that you have a high amount of fat and cholesterol deposits coursing through your blood vessels that can accumulate and block the vessels. When that happens, you run a high risk for cardiovascular diseases such as heart attacks and strokes.
“Lowering cholesterol levels reduces the risk of such events,” said Prof Tan.
And what about statins’ contribution? “In the high-risk populations studied, those who took statins had 20 per cent to 40 per cent fewer heart attacks, strokes and deaths than those who did not over two to five years,” said Prof Tan.
“Statin therapy is also the standard of care for patients with peripheral artery disease (that is, blockages that occur in the lower limb arteries) in all the international guidelines.”

