Stomach aches and diarrhoea: How can we tell if it’s food poisoning, IBS or inflammatory bowel disease?
How do you tell if that stomach ache and diarrhoea are from last night's dodgy dinner, irritable bowel syndrome (IBS) or an inflammatory bowel disease (IBD) such as Crohn's disease or ulcerative colitis?

(Photo: iStock/Sitthiphong)

This audio is generated by an AI tool.


With our love for food and penchant for food hunting (sometimes on dubious grounds), ingesting the odd tummy-upsetting pathogen is almost par for the course – along with a bout or two of abdominal discomfort, diarrhoea or changes in bowel habits.
But what if that stomach pain means more than just a case of food poisoning because, as it turns out, there are many other bowel conditions that can also elicit similar reactions?
For example, irritable bowel syndrome or IBS is always characterised by abdominal pain after eating, though it may also be accompanied with diarrhoea, constipation or a change in stool consistency, said Dr Eric Wee, a senior consultant gastroenterologist with Nobel Gastroenterology Centre at Mount Elizabeth Novena Hospital.
Another gastrointestinal issue, inflammatory bowel disease or IBD, may also share similar symptoms.

“Many patients consult gastroenterologists thinking they might have an IBD or IBS, and are eventually diagnosed to have the other condition, or some other illness such as a gastroenteritis (infection) instead,” said Dr Wee.
“Much of the confusion stems from the fact that both conditions may present with abdominal pain, diarrhoea or a change in the bowel habit. The more serious condition is IBD and fortunately, it occurs infrequently.”
HOW DO WE TELL IF IT’S JUST FOOD POISONING OR SOMETHING ELSE?
It can be difficult to tell because diarrhoea, stomach pain and bloating are signs of many digestive diseases, including IBS, IBD, celiac disease, gluten intolerance and lactose intolerance, according to Dr Wee, who said the most common cause is usually food poisoning or gastroenteritis.
IBS refers to a functional condition where the digestive system is over-sensitive to different triggers that cause it to move too fast or too slowly, resulting in diarrhoea or constipation, and often in association with abdominal pain, said Dr Melvin Look, the director of PanAsia Surgery in Mount Elizabeth Hospital, Mount Elizabeth Novena Hospital and Parkway East Hospital.
The reasons for the excessive muscle contractions are often not completely understood, according to Singhealth, although they can include “diet intolerance, stress, depression, abnormality in intestinal bacteria content or abnormal intestinal tract movement”.

There is ground to suspect IBS if your abdominal pain or discomfort persists for at least three days per month in the last three months – and is accompanied by at least two of the following:
- Pain improves after passing motion
- Changes in the frequency of passing motion
- Changes in stool form
IBD is another tough one to know for sure. “There are no unique symptoms for IBD”, said Dr Wee. “However, patients often have mucous and blood in their stools. Their symptoms tend to have a longer and more chronic history as compared to gastroenteritis, which hits an individual relatively hard and fast. In severe cases of IBD, there may be fatigue, anaemia, fever and weight loss.”
SO, IS THAT IBS OR IBD?
One way to know what you have is through medical tests such as scans, stool tests, colonoscopies and biopsies. For IBS, “biopsies of the bowel generally do not show any abnormality”, said Dr Sulaiman Bin Yusof, a colorectal and general surgeon with Colorectal Clinic Associates. In contrast, IBD biopsies often show up distinct abnormalities, he said.
IBD is an autoimmune disease caused by the inflammation of the digestive tract, explained Dr Wee. “Immune cells from the body inadvertently cause damage to the digestive tract.” Depending on which part of the gastrointestinal tract is affected, IBD is categorised as Crohn’s disease or ulcerative colitis.
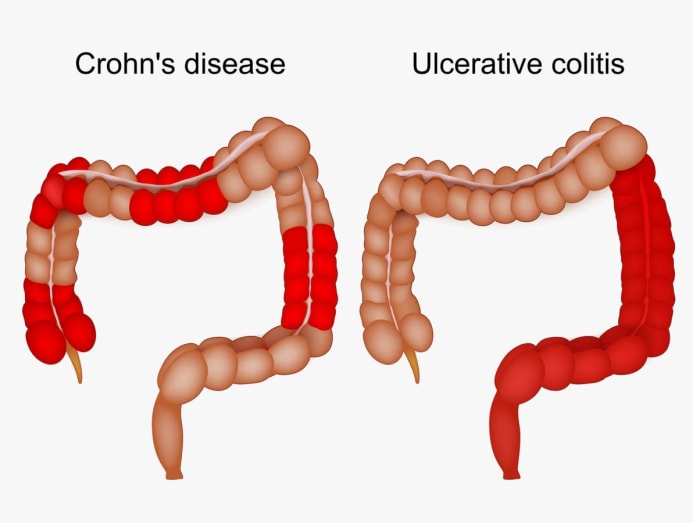
In Crohn’s disease, the mouth, oesophagus, stomach, small bowel, colon and anus can be affected. The damaged areas may appear in patches that are next to areas of healthy tissue, according to the US Centers for Disease Control and Prevention.
“Crohn’s disease may affect one location in the digestive tract or multiple places simultaneously,” said Dr Wee. “In severe cases, the inflammation may extend through the bowel wall and into other organs or the skin.”
Meanwhile, ulcerative colitis mainly affects the large intestine or colon, said Dr Sulaiman. “In some cases, ulcerative colitis can also affect the last part of the small intestine before it joins the colon. Typically, ulcerative colitis affects the left side of the colon and rectum. Its hallmark feature is continuous areas of shallow ulceration of the colon.”
Both of these conditions may also manifest with joint pain in the knee or elbow, added Dr Wee.
Why aren’t celiac disease, gluten intolerance and lactose intolerance considered IBDs?
They are primarily due to the gastrointestinal tract's inability to process and digest certain foods such gluten or lactose, said Dr Melvin Look, the director of PanAsia Surgery in Mount Elizabeth Hospital, Mount Elizabeth Novena Hospital and Parkway East Hospital. "They do not cause chronic inflammation of the bowels and are not considered to be IBDs," he said.
HOW COMMON ARE IBS AND IBD IN SINGAPORE?
Nearly one in 10 Singaporeans suffers from IBS, according to HealthXchange. When it comes to IBD, the number is lower. "Currently, it is estimated that there are 1,500 individuals who may be suffering from IBD in Singapore, of which 200 are children," said Dr Sulaiman.
While low, IBD cases appear to be on the rise. “Singapore General Hospital saw close to 600 patients diagnosed with the disease in the year 2017, a two-fold increase from a decade ago in 2007,” said Dr Sulaiman, citing press reports. “National University Hospital saw a striking eight-fold increase in IBD patients, from below 50 in 2013 to close to 400 cases in 2018. The rise in numbers can be attributed to better awareness and better diagnostic capabilities in recent years.”
Of the two IBD conditions, “ulcerative colitis is more common than Crohn’s disease and fortunately, ulcerative colitis is easier to treat”, said Dr Wee. “Crohn’s disease has more complications and is more resistant to treatment.”

WHAT ARE THE POSSIBLE REPERCUSSIONS OF IBS AND IBD?
When it comes to IBD, one word: Cancer – or more specifically, colorectal cancer. In Crohn’s disease that only affects the small intestine, it may also cause cancer in that part of your gastrointestinal system, said Dr Sulaiman.
Added Dr Look: “Patients with ulcerative colitis, for example, have four to 10 times the risk of developing colorectal cancer".
“The constant inflammation results in a high cell turnover, which predisposes to mutations resulting in cancer,” explained Dr Wee. “Other factors include increased oxidative stress from the inflammation that leads to changes in the genes driving mutation.” Even the changes the gut microbiota undergo, owing to the medicines used to treat the autoimmune disease, may increase cancer risk, he said.
Unlike IBD, IBS does not cause inflammation, a key factor in colorectal cancer risk.
ARE DIARRHOEA AND FREQUENT BOWEL MOVEMENTS THE SAME?
The two are not interchangeable. "Diarrhoea" refers to the texture and consistency of the stools, which are often "watery", "lack form" and are "mushy or purely liquid", explained Dr Eric Wee, a senior consultant gastroenterologist with Nobel Gastroenterology Centre at Mount Elizabeth Novena Hospital.
"Frequent bowel movements" refers to an excessive number of bowel movements a day, said Dr Wee. There isn't a “normal” number of daily bowel movements as it varies from person to person. But it generally refers to defecating more often than you usually do. "Frequent bowel movements need not always mean passing soft, watery stools. It can also include normal or even hard stools," said Dr Wee.
WHAT ARE THE TREATMENTS AVAILABLE?
There may be a myriad of IBS treatments out there but research that backs their effectiveness remains to be seen. Here are some, according to studies:
- Peppermint oil: It supposedly calms the intestine by relaxing its muscles. Research suggests taking 500mg to 800mg per day in capsules.
- Probiotics: Introducing beneficial gut bacteria may help. However, experts have yet to determine the bacteria type and dose.
- Anti-cramping medications: They relieve pain by relaxing the muscles of the intestine but may create side effects such as dry mouth, dizziness and blurred vision.
- Cognitive behavioural therapy: It is thought that stress may contribute to IBS and there is some evidence that such therapy may help.

When it comes to IBD such as Crohn’s disease and ulcerative colitis, patients are usually treated with medicines that control the immune system, said Dr Wee, citing tablets and monthly injections. “There are many modern treatment options available and they include classes of drugs such as steroids, aminosalicylates, immunomodulators, biologic therapies, small molecule drugs and JAK inhibitors."
Medicines aside, manipulating your diet may also help IBD, said Dr Wee, citing data from clinical trials. That means avoiding triggering foods such as processed food, preservatives, artificial sweeteners and emulsifiers as well as minimising gluten, dairy and alcohol.
“Complete avoidance is not mandatory but one needs to exercise restraint. Limiting the intake of red meat is believed to be important, too,” said Dr Wee. Unfortunately, changing your diet alone is often not adequate. “Almost all individuals with IBD will require medical treatment concurrently.”
Surgery to remove the affected gastrointestinal parts is only used when medical therapy fails, said Dr Sulaiman. For instance, surgery may be used to manage the complications from Crohn’s disease to preserve as much of the bowel as possible.